If you have been battling a stubborn tendon or soft-tissue pain that will not settle, shockwave therapy may be the thing that helps you turn the corner. It is a non-invasive treatment that restarts a stalled healing response, and I use it as part of a plan built around your specific problem, paired with the exercise that rebuilds the tissue so the result lasts. The first step is a proper assessment, so we both know it is the right tool for you before we begin.
Shockwave is most useful for long-standing problems that have not eased with time and basic care, usually pain that has been there for several weeks or longer. You might recognise some of these:
My background is in interdisciplinary pain management, and I use shockwave the way I use any tool, as one part of a plan rather than a fix on its own. The conditions it helps most are long-standing tendon and fascia problems, and those recover when we gradually rebuild the tissue's capacity to handle load. Shockwave gets that process moving again. It calms the pain enough for you to start loading, restarts a healing response that has stalled, and speeds things up when it is paired with the right exercise.
That is why I assess first, and why almost everyone I treat is given specific exercises to do alongside their sessions. The best results in the research come from shockwave and loading together, and that combination is what gives you a lasting result rather than short-lived relief.
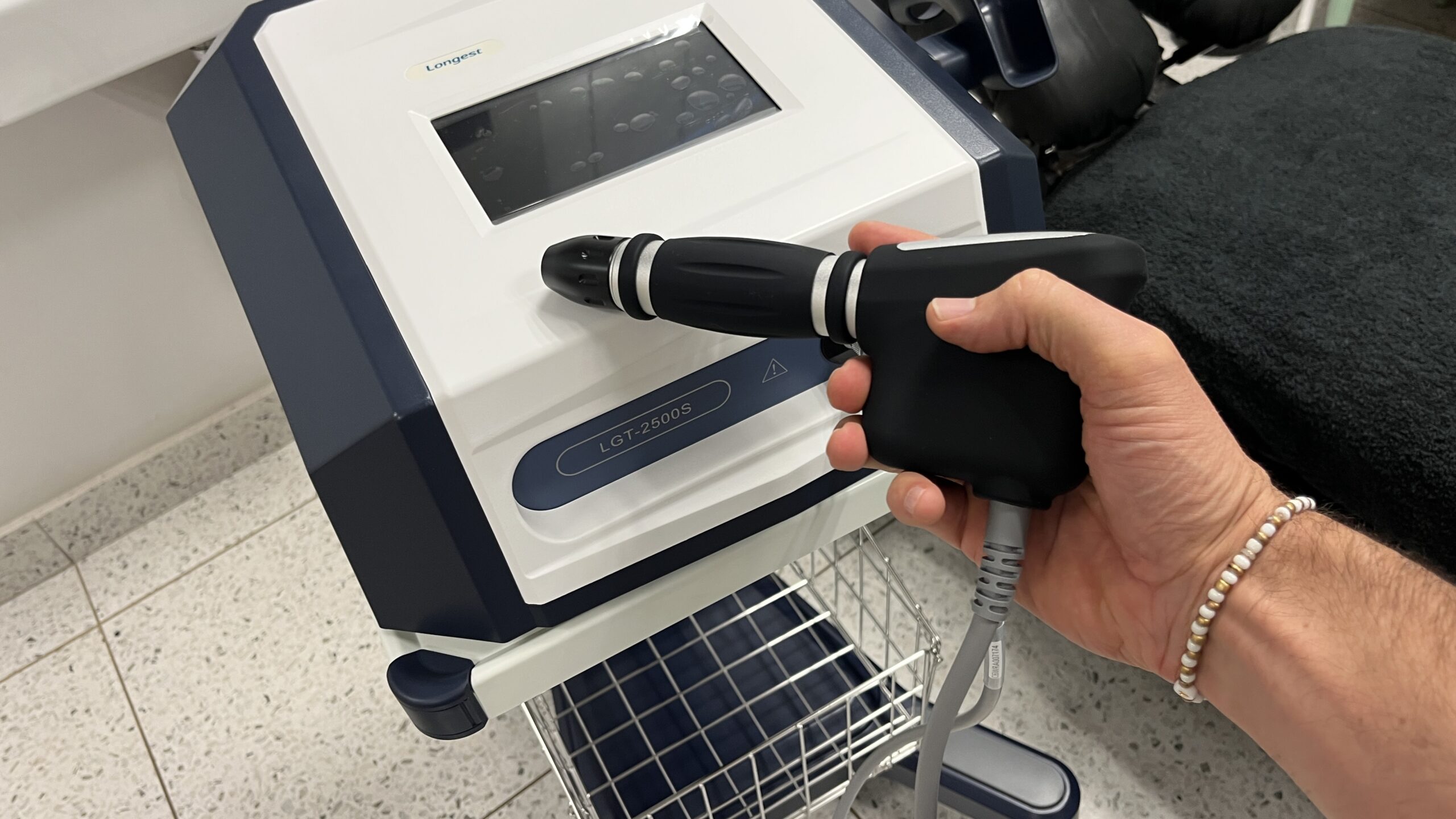
Shockwave therapy delivers pressure waves into the affected tissue through a handpiece held against the skin. Those waves carry mechanical energy into the target, and that energy sets off a sequence of responses in the body.
There is no injection, no anaesthetic, and no incision. I use a radial shockwave unit (Longest D-Actor HP), which is well suited to the tendon and fascia problems shockwave treats best.
These are the problems I see shockwave help with most. Many of the people I treat have already tried other things without much luck, so if you recognise your pain here, there is good reason to be hopeful.
This is the problem shockwave helps with most reliably. For heel pain that has not settled with stretching and load changes, there is good evidence for meaningful relief, delivered alongside a calf and foot loading programme.
Read more →For chronic outer-elbow pain, shockwave reduces pain and improves grip strength. It is slower to act than a cortisone injection in the first month but clearly better at three to six months.
Read more →For pain on the outside of the hip, the landmark trial used radial shockwave and found it outperformed a cortisone injection over the medium and long term. It works best with a gluteal strengthening programme.
Read more →A frustrating problem that many clinics struggle to help with, but one with direct trial support in athletes. If you are a runner with deep pain at the sitting bone, this is worth a conversation.
Read more →For calcium deposits in the rotator cuff tendons, shockwave is one of the better non-surgical options, helping break down and reabsorb the deposit while easing the pain.
Read more →Many of the people I see are runners and cyclists. Shockwave has a supporting role in midportion Achilles tendinopathy and in shin splints, where I always assess to rule out a stress fracture first.
Treatment is a short course rather than a single visit, usually around three to six weekly sessions depending on the condition and how you respond. Each session is quick, often only a few minutes of actual treatment once the area is located, with a gel applied at the contact point.
The sensation is firm and can be briefly uncomfortable, because the treatment works by sending pressure waves into the tissue. I set the intensity to a level you can tolerate, and most people describe it as a strong tapping that is bearable and short. There is very little downtime. Some tenderness, redness, or an occasional small bruise for a day or two is normal, and I will guide you on how to load the area sensibly between sessions. Many people feel some relief early, and the deeper tissue changes build over the following weeks, so we judge the fuller result a month or more after the course rather than on the day.
Shockwave is not the answer to every problem, and part of my job is making sure it is the right fit before we start. It works best for pain that has been around for a while, so for a fresh injury there are usually better first steps. And because it works alongside exercise rather than instead of it, you will always leave with a plan, not just a course of treatment. Now and then the assessment turns up something that needs a different approach altogether, such as a stress fracture behaving like shin splints, and catching that early is exactly the point of starting with a proper look.
There are also a few situations where shockwave is best avoided for safety, including during pregnancy, if you are on blood-thinning medication, or near a pacemaker. I check all of this with you first, so you can feel confident the treatment is both suitable and safe.

Dr Neil Cuninghame is a chiropractor and interdisciplinary pain management specialist practising in Hillcrest. He holds an MTech in Chiropractic from the Durban University of Technology and a Postgraduate Diploma in Interdisciplinary Pain Management from the University of Cape Town, and has more than 17 years of clinical experience. His pain-management background is the reason he uses shockwave as one part of a plan rather than a treatment on its own.
It is firm and can be briefly uncomfortable, because the treatment works by sending pressure waves into the tissue. I set the intensity to a level you can tolerate, the treatment itself is short, and most people manage it comfortably.
Most conditions are treated with a short course of roughly three to six weekly sessions, adjusted to how you respond. Some relief often comes early, while the fuller benefit builds over the weeks after the course.
Very little. You can usually carry on with normal daily activity, with some mild tenderness, redness, or occasional bruising in the treated area for a day or two.
The strongest evidence is for plantar heel pain, lateral hip and gluteal tendon pain, tennis elbow, proximal hamstring tendinopathy, and calcific shoulder problems, with useful roles in several other tendon conditions when combined with the right exercise.
Yes, for a defined set of conditions. I offer shockwave where good-quality trials and reviews support it, and I am upfront where the evidence is weaker, rather than promoting it for everything.
No. Shockwave works best alongside a loading programme. It reduces pain and restarts healing so that the exercise that ultimately rebuilds the tissue becomes possible and more effective.
For several conditions it is a reasonable step to try before more invasive options, and for tennis elbow in particular it tends to outperform a cortisone injection over the longer term.
Most people can. It is avoided in pregnancy over the trunk and pelvis, in those on blood thinners or with bleeding disorders, near pacemakers, over tumours or infections, and over children's growth plates. I check your suitability before treatment.
If you have been battling a stubborn tendon or soft-tissue pain, you do not have to simply put up with it. The first step is an assessment, so we can work out whether shockwave is the right tool for you and how it fits into your treatment plan.